What It's Like to Be a Mobile PT with PT Near Me
A realistic day-in-the-life of a Florida mobile physical therapist: 4–6 in-home visits, one-on-one care, post-MVA caseload, no productivity quotas, and the autonomy to actually treat.
Andre Bennett, PT, DPT
Senior Clinician
The first time you skip the parking lot
The honest pitch for mobile work isn't the pay or the flexibility — those matter, but they're downstream. The thing that hooks most clinicians is the first morning they realize they're not driving to a building. They're driving to a person. There's no badge to scan, no waiting room to walk through, no front desk asking if you can squeeze in one more eval. You park, you knock, you treat.
This post is for PTs (and PTAs — there's a separate post for you) who are curious what a mobile day actually looks like inside the PT Near Me model. Not the marketing version. The real version: the driving, the documentation, the post-MVA caseload, the things that are great, and the things you should know before you sign anything.
A realistic day: 4–6 visits, one cluster, one patient at a time
Most full-time mobile PTs in our network run 4–6 visits a day. Some PRN clinicians do 2–3. The schedule is built around a geographic cluster, not a clock — we route your day so you're not crisscrossing the metro.
A typical Tuesday in, say, the Brandon/Riverview area might look like this:
- 8:30 AM — Eval, 62-year-old, rear-end collision 9 days post-crash, neck + low back. 60–75 minutes including the first treatment.
- 10:15 AM — Follow-up, 28-year-old, post-MVA shoulder, visit 6 of 12.
- 11:30 AM — Follow-up, 71-year-old, post-MVA knee, visit 4. Note for the referring physician.
- 1:30 PM — Eval, 45-year-old, T-bone collision, second opinion on whiplash + headache.
- 3:00 PM — Follow-up, 19-year-old, post-MVA lumbar, near discharge.
- Done by 4:30. Documentation finished by 5:15.
That's it. No 7:00 PM patients to backfill a quota. No double-booked evals. No co-treating with a tech you've never met. The pace is real work — driving plus treatment plus notes — but it isn't the frantic high-volume churn most clinicians left the clinic to escape.
What an in-home visit is actually like
In-home is not a stripped-down clinic visit. It's a different format. You bring a goniometer, a couple of bands, a few cuff weights or a sandbag, and your hands. The kitchen counter becomes the parallel bar. The hallway becomes the gait lab. The staircase becomes the closed-chain progression.
What you gain is enormous: you see the actual environment the patient has to function in. You watch a post-MVA patient navigate the exact transfer that's been waking them up at 3 AM. You meet the spouse. You see the medication pile on the counter. You catch the throw rug they're going to trip on. You finish with a HEP that uses the chair they actually sit in, not a generic handout.
The caseload: post-MVA, motivated, early-phase
Nearly every patient on your caseload is recovering from a Florida auto accident and being billed under Personal Injury Protection (PIP). That has practical implications for how you practice:
- Patients come to you fast. Florida Statute § 627.736 requires initial care within 14 days of the crash. That means you see people early — when good PT actually changes the trajectory.
- They're motivated. They're in pain, they're worried about long-term function, and they want to get back to driving, working, and parenting.
- The orthopedic picture is familiar: cervical and lumbar strain, whiplash-associated disorders, shoulder and knee mechanics from bracing on impact, post-concussive symptoms, and the occasional post-surgical hand-off.
- There's a real referral pipeline. You're not hustling for evals — they come in through physicians, urgent cares, and direct intake.
The research case for early PT is also strong, and it's the reason this model exists. Studies of low back pain show that getting patients into PT within 14 days of onset is associated with sharply lower downstream utilization — fewer opioid prescriptions, fewer advanced images, fewer injections, fewer ED visits, and lower total spend over the following year. That's the clinical lane we live in.
The autonomy — what you actually get to control
If you've worked in a high-volume outpatient clinic, the word "autonomy" has probably been used in a job posting that meant the opposite. Here's what it means in this model, concretely:
- Your hours. You set your availability week by week. Want Fridays off? Block Fridays. Want only mornings? Take only mornings. Want a full caseload? Open the calendar.
- Your geographic radius. You define how far you're willing to drive. We don't route you outside it.
- Your plan of care. You're the licensed clinician — you write the eval, set the frequency, progress the program, and decide when the patient is ready for discharge. No productivity dashboard is grading you.
- Your treatment style. Manual-heavy, exercise-heavy, education-heavy — your call. We care about outcomes and documentation, not which technique you prefer.
What PT Near Me handles so you can practice
The reason this model works as a 1099 arrangement is that the back office is real. You're not running a private practice from your car. You're a credentialed clinician on a platform that handles the parts of practice that drain clinicians dry:
- Intake and scheduling — patients are screened, eligibility is verified, and visits are routed to you in your radius.
- PIP and MedPay billing — we bill the auto policy directly. You document; we collect.
- Compliance scaffolding — note templates, signatures, frequency justifications, and the documentation flow that PIP carriers actually want to see.
- Physician communication — initial evals and progress notes routed to the referring provider on the cadence they expect.
- Marketing and referrals — you don't need to court physician offices on your lunch break.
The honest tradeoffs
Mobile, 1099, in-home work isn't the right fit for everyone. The clinicians who thrive in this model tend to share a few traits, and the ones who struggle usually struggle for predictable reasons.
It's a great fit if you: like driving and being alone between visits, want to control your schedule, value clinical autonomy more than benefits, are comfortable with self-employment taxes, and want a one-on-one caseload.
It's a harder fit if you: want guaranteed W-2 hours and employer-paid health insurance, prefer a team-based clinic environment all day, dislike driving, or want someone else to set your daily schedule for you.
If this sounds like the next chapter of your career
If the day above sounds like a relief instead of a stretch, that's usually the signal. The next step is to read how the 1099 model works financially, look at the licensing and credentialing side, and then apply when you're ready.
Frequently asked questions
- How many patients will I see per day?
- Most full-time mobile PTs run 4–6 in-home visits a day in a tight geographic cluster. PRN clinicians often run 2–3. You set your own availability and radius, so the daily count is ultimately your call.
- Do I need my own equipment?
- A basic in-home kit — goniometer, resistance bands, a few cuff weights or a small sandbag, gait belt, BP cuff and pulse ox — covers the vast majority of post-MVA orthopedic care. You'll dial in the rest within the first month.
- What kinds of patients will I treat?
- Almost entirely Florida auto-accident patients in the early phase of recovery: cervical and lumbar strain, whiplash, shoulder and knee mechanics from the crash, post-concussive symptoms, and occasional post-surgical hand-offs.
- Is this employment or contracting?
- Contracting. Clinicians in the PT Near Me network are independent (1099) contractors. You own your schedule and your business; we provide the platform, the referrals, the billing, and the back office.
- Do I have to take a minimum number of visits?
- No. You set your own availability — anywhere from a few PRN visits a week to a full caseload.
Related articles
- Life as a PT/PTA with PT Near Me
PT vs. PTA on an In-Home Auto-Injury Team: How the Roles Work Together
The PT writes the eval and plan of care; the PTA delivers ongoing treatment under that plan. In a mobile auto-injury setting, the partnership is closer and more efficient than most clinic models — here's how it actually works.
Dr. Sam Rose, PT, DPT · June 21, 2026
- Life as a PT/PTA with PT Near Me
How 1099 Per-Visit Pay Works for In-Home Physical Therapists
1099 per-visit pay means you're paid for completed visits as an independent contractor — not for hours, not for productivity dashboards. Here's how it actually works for in-home PTs, including the tax and flexibility tradeoffs to understand before you sign.
Dr. Sam Rose, PT, DPT · June 22, 2026
- Life as a PT/PTA with PT Near Me
Designing Your Week as a 1099 PT: PRN, Part-Time, or a Full Caseload
One of the real advantages of contractor work is that you design the week — PRN, part-time around a W-2 role, or a full mobile caseload. Here's how each pattern actually looks for in-home PTs and PTAs.
Andre Bennett, PT, DPT · June 25, 2026
In your city
Conditions we treat across Florida
Each city page below covers the clinical evidence, recovery timelines, and PIP details specific to these conditions.
- Whiplash — Tampa
- Whiplash — Orlando
- Whiplash — Miami
- Whiplash — St. Petersburg
- Low Back Pain — Tampa
- Low Back Pain — Orlando
- Low Back Pain — Miami
- Low Back Pain — St. Petersburg
- Concussion — Tampa
- Concussion — Orlando
- Concussion — Miami
- Concussion — St. Petersburg
- Shoulder Injury — Tampa
- Shoulder Injury — Orlando
- Shoulder Injury — Miami
- Shoulder Injury — St. Petersburg
Don’t see your city? View all Florida service areas.
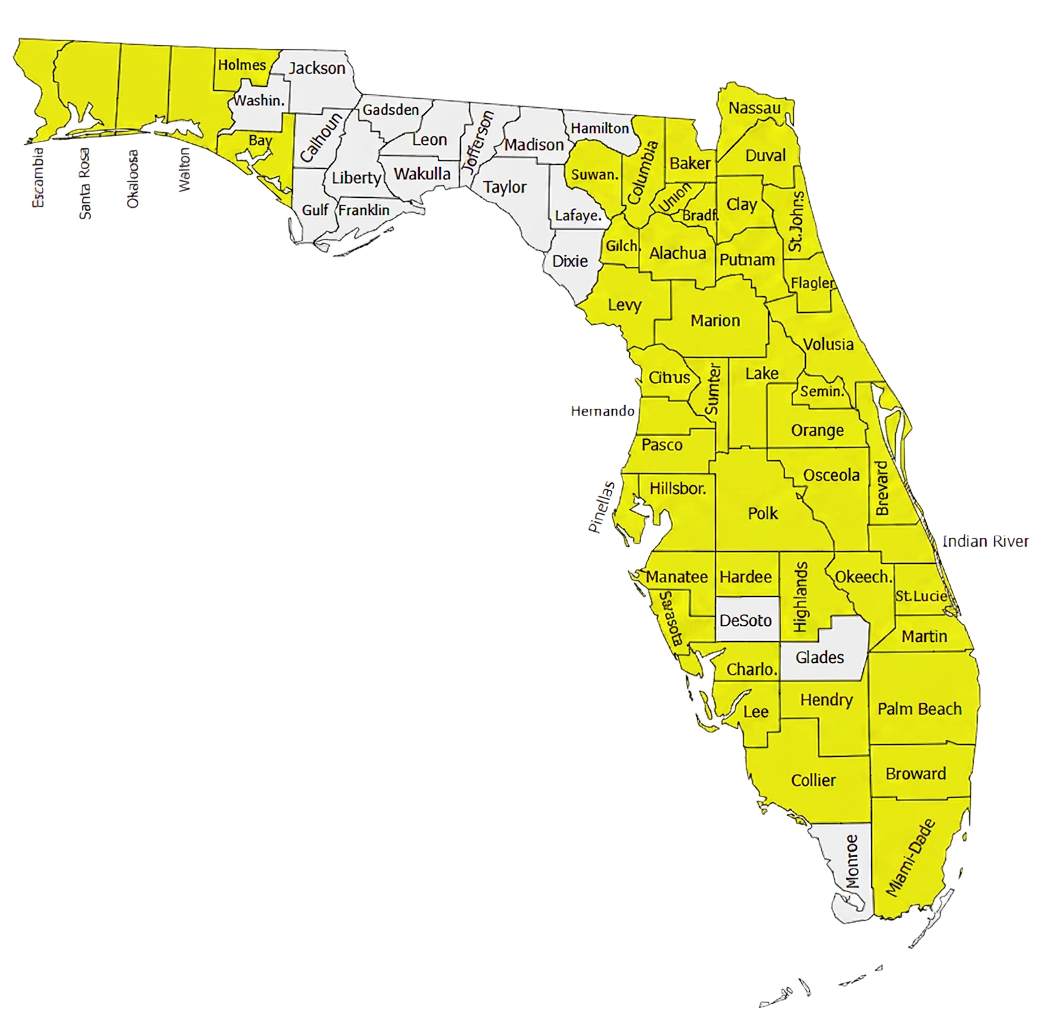
500+ Physical Therapists covering 35+ counties in Florida.
Our clinician network reaches major metros and rural communities alike — from the Panhandle to the Keys. If a patient is in a highlighted county, we can usually see them at home within 24–72 hours of intake.
- Clinicians in network
- 500+
- Florida counties covered
- 35+
Need to refer a Florida patient?
Our intake team confirms PIP and MedPay coverage during the call and schedules most patients for an in-home evaluation within 48 hours.