PT vs. PTA on an In-Home Auto-Injury Team: How the Roles Work Together
The PT writes the eval and plan of care; the PTA delivers ongoing treatment under that plan. In a mobile auto-injury setting, the partnership is closer and more efficient than most clinic models — here's how it actually works.
Dr. Sam Rose, PT, DPT
Clinical Director, PT Near Me
Why this question matters in a mobile setting
In a busy outpatient clinic, the line between what the PT does and what the PTA does can blur. Same gym. Same equipment. Same patient passed back and forth across the room. In a mobile, in-home model the roles get clearer, not muddier — because every visit is a single clinician with a single patient. You can't hand off mid-set. The plan of care, the documentation, and the handoffs have to actually function.
If you're a PT thinking about adding a PTA to your patients' care, or a PTA evaluating whether the mobile auto-injury world is a place you can thrive, here's how the two roles actually work together inside the PT Near Me model.
Scope at a glance
| Task | PT (DPT) | PTA |
|---|---|---|
| Initial evaluation | Yes | No |
| Plan of care (POC) | Yes — writes and signs | No — works under POC |
| Re-evaluations | Yes | No |
| Treatment per established POC | Yes | Yes |
| Progress documentation | Yes | Yes (within scope) |
| Discharge summary | Yes | No |
| Plan-of-care changes | Yes | Recommends to supervising PT |
| Supervision of PTA | Yes | — |
This isn't a hierarchy of skill. It's a regulatory and clinical division of responsibility. The PT is accountable for the diagnostic reasoning and the trajectory of the case. The PTA is accountable for delivering high-quality, patient-specific treatment within that plan.
What Florida actually requires
Florida's Physical Therapy Practice Act (Chapter 486) and the Board of Physical Therapy rules define PTA practice as treatment delivered under the direction and supervision of a Florida-licensed PT. The supervising PT is clinically responsible for the patient. The day-to-day supervision model — direct, on-site, or general — varies by setting; in mobile in-home care the PT is reachable in real time and re-engages the case at re-evals and at any point the PTA flags a change.
What this looks like on an auto-injury caseload
A typical PIP-covered patient might have an episode of care that runs 8–16 visits across 4–8 weeks. The PT/PTA partnership shapes that arc:
- PT performs the initial evaluation in the home. 60–75 minutes. Sets diagnosis, prognosis, frequency, goals, and the first phase of the plan.
- Plan of care signed and routed to the referring physician.
- PTA picks up treatment visits 2–N, executing the program — manual techniques within scope, therapeutic exercise progression, neuromuscular re-education, HEP reinforcement, environmental modification.
- PT re-evaluates at the regulatory and clinical inflection points (typically every ~10 visits or 30 days, sooner if status changes).
- PT writes the discharge summary and final note for the physician.
The patient experiences this as continuity, not handoff. They know which clinician is the PT and which is the PTA, but they get the same plan, the same goals, and the same HEP across the episode.
What this is like for the PTA
The most common thing PTAs tell us after a few weeks in the mobile model: they didn't realize how much of their clinic day used to disappear into setup, room turnover, and tech overflow. In-home, every minute of the visit is hands-on with the patient.
- One-on-one, every visit. No three-patient-deep gym shuffle.
- A motivated post-MVA caseload. People who want to get back to driving, working, and parenting.
- A supervising PT who's actually available, because they're carrying their own active caseload — not running an admin role.
- Real progression — you watch a patient go from "can't sleep on that shoulder" to driving and lifting a toddler again.
- 1099 schedule control. Open the days you want to work; close the ones you don't.
What this is like for the supervising PT
PTs in our network who work with a PTA on shared patients usually describe the workflow as cleaner than what they had in the clinic. You write the eval, set the plan, and trust the PTA to execute. You re-engage at re-evals and at any flagged change. You're not co-treating in the same room or wrestling over schedule conflicts.
It also expands what you can take on. A solo PT has a hard ceiling on visit volume — there are only so many evaluations you can do in a week. With a PTA executing the middle of the plan, you can accept more new evals without compromising care.
The handoff that makes or breaks the model
Mobile PT/PTA collaboration only works if three things are true:
- The initial eval is detailed enough that the PTA can execute without guessing.
- Communication is fast — same-day for anything clinically meaningful.
- The documentation system makes it easy for the PT to see what the PTA did, and easy for the PTA to see what the PT planned.
That's what the platform side of PT Near Me is built to support. Templates, signed plans of care, shared notes, and a re-eval cadence that's already on the calendar.
Where to go from here
Frequently asked questions
- Can a PTA perform the initial evaluation?
- No. Under Florida law, the initial evaluation, plan of care, re-evaluation, and discharge must be performed and signed by a licensed PT. PTAs deliver treatment under that established plan.
- Does the PT have to be physically present when the PTA treats?
- Not in the in-home model. Florida allows general supervision for outpatient settings, meaning the supervising PT must be available — typically by phone or video — and re-engages the case at clinically appropriate intervals. Our model uses scheduled re-evals plus same-day communication on any flagged change.
- Do PTAs make less than PTs in this model?
- Per-visit rates are set by role and reflect the regulatory scope. We don't publish rate figures publicly — those are part of the contracting conversation. The platform, the back office, and the schedule control are the same for both.
- Can a PTA carry their own caseload of patients?
- Yes — within the plan of care set by the supervising PT. Most PTAs in our network see a stable mix of follow-up visits across several active episodes of care.
Related articles
- Life as a PT/PTA with PT Near Me
What It's Like to Be a Mobile PT with PT Near Me
A realistic day-in-the-life of a Florida mobile physical therapist: 4–6 in-home visits, one-on-one care, post-MVA caseload, no productivity quotas, and the autonomy to actually treat.
Andre Bennett, PT, DPT · June 20, 2026
- Life as a PT/PTA with PT Near Me
How to Become a Mobile PT or PTA in Florida
A step-by-step guide to becoming a mobile, in-home physical therapist or PTA in Florida — licensure with the Florida Board of Physical Therapy, the credentials you'll need to contract, and how to actually start taking visits.
Andre Bennett, PT, DPT · June 23, 2026
- PT Basics & Glossary
Physical Therapist vs. PTA: Roles, Education, and Differences
PTs and PTAs both treat patients, but they aren't interchangeable. A clear look at scope, education, and what each role does during your care.
Dr. Sam Rose, PT, DPT · June 22, 2026
In your city
Conditions we treat across Florida
Each city page below covers the clinical evidence, recovery timelines, and PIP details specific to these conditions.
- Whiplash — Tampa
- Whiplash — Orlando
- Whiplash — Miami
- Whiplash — St. Petersburg
- Low Back Pain — Tampa
- Low Back Pain — Orlando
- Low Back Pain — Miami
- Low Back Pain — St. Petersburg
- Concussion — Tampa
- Concussion — Orlando
- Concussion — Miami
- Concussion — St. Petersburg
- Shoulder Injury — Tampa
- Shoulder Injury — Orlando
- Shoulder Injury — Miami
- Shoulder Injury — St. Petersburg
Don’t see your city? View all Florida service areas.
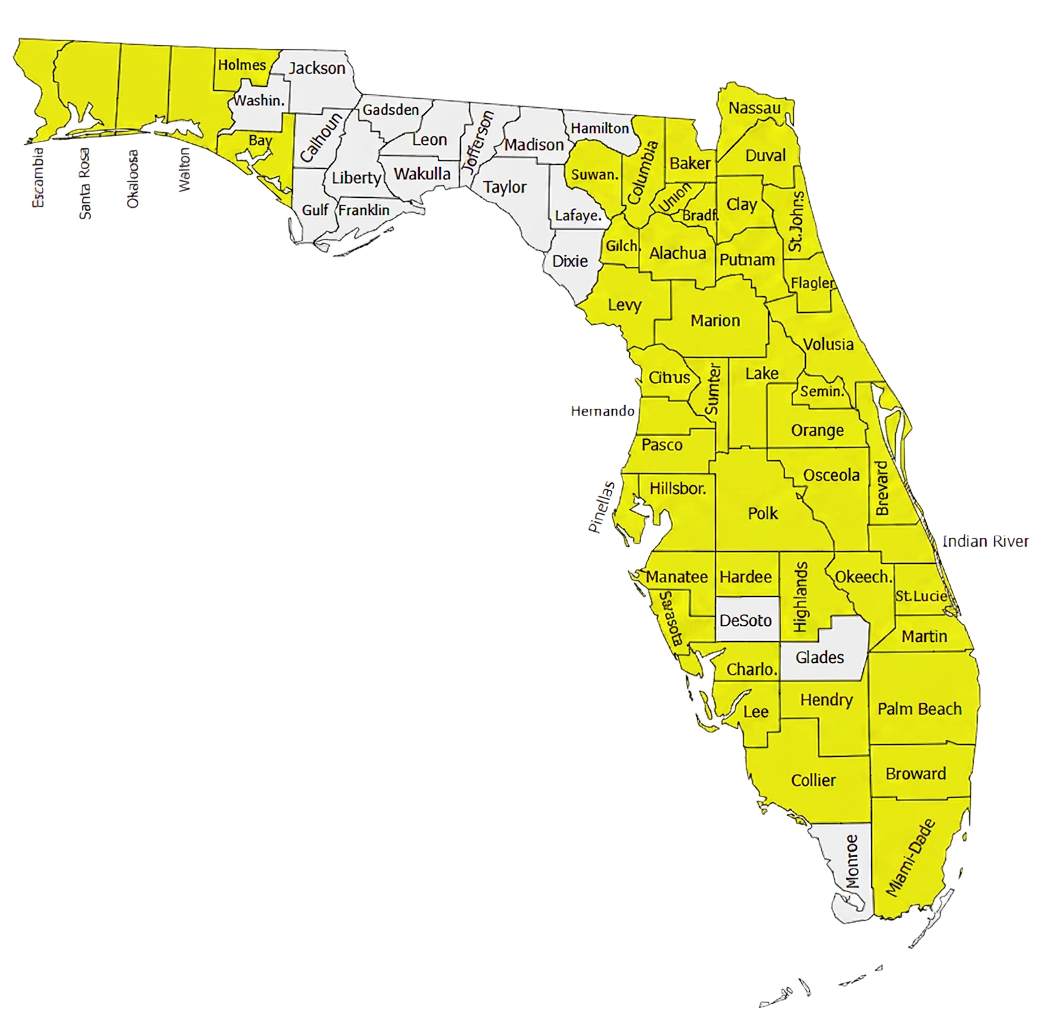
500+ Physical Therapists covering 35+ counties in Florida.
Our clinician network reaches major metros and rural communities alike — from the Panhandle to the Keys. If a patient is in a highlighted county, we can usually see them at home within 24–72 hours of intake.
- Clinicians in network
- 500+
- Florida counties covered
- 35+
Need to refer a Florida patient?
Our intake team confirms PIP and MedPay coverage during the call and schedules most patients for an in-home evaluation within 48 hours.