Whiplash After a Florida Car Accident: What to Expect in Recovery
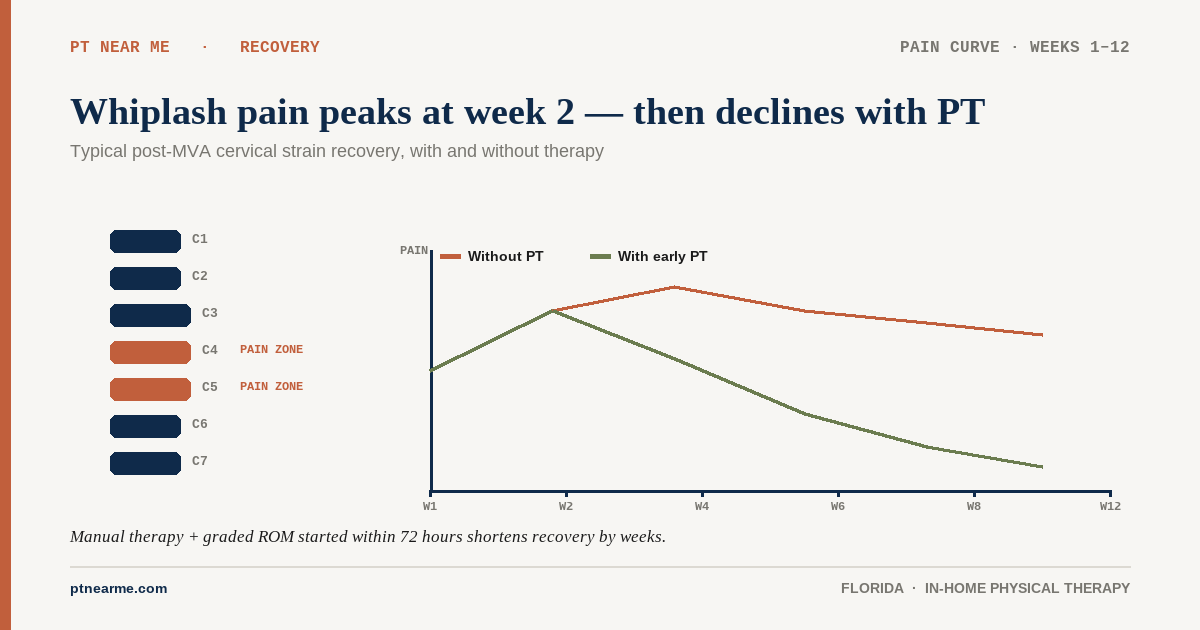
Most whiplash recovers within 6 to 12 weeks with early, active physical therapy. A smaller share develops persistent symptoms past three months. Here's what whiplash actually is, what the realistic timeline looks like, and how PT should approach it after a crash in Florida.
Andre Bennett, PT, DPT
Senior Clinician
What whiplash actually is
Whiplash — clinically, whiplash-associated disorder (WAD) — is the cluster of neck symptoms that follow a sudden acceleration-deceleration of the head, most often in a rear-end collision. The mechanism stretches and strains the cervical muscles, ligaments, and joint capsules. Most cases involve no fracture and no nerve damage; the injury is to soft tissue.
Common symptoms in the first 72 hours include neck pain and stiffness, headaches (often starting at the base of the skull), restricted range of motion, upper-back tightness, and sometimes dizziness or jaw soreness. Symptoms frequently peak 24 to 72 hours after the crash, not at the scene — which is one reason patients often underestimate the injury initially.
How whiplash is graded
Clinicians use the Quebec Task Force grading system to classify WAD by severity:
| Grade | Findings | Typical course |
|---|---|---|
| WAD 0 | No neck complaints, no physical signs. | No treatment indicated. |
| WAD I | Neck pain, stiffness, or tenderness only. No physical signs. | Generally resolves in days to weeks with activity and reassurance. |
| WAD II | Neck complaints AND musculoskeletal signs (decreased range of motion, point tenderness). | Most common presentation. 6–12 weeks with structured PT in most patients. |
| WAD III | Neck complaints AND neurological signs (decreased deep tendon reflexes, weakness, sensory deficits). | Longer course; requires physician co-management. PT still indicated. |
| WAD IV | Neck complaints AND fracture or dislocation. | Surgical evaluation; PT after stabilization. |
The overwhelming majority of post-MVA whiplash referrals fall into WAD I and II. Those are the cases where early active PT produces the biggest functional gains.
A realistic recovery timeline
Week 1–2: pain control and gentle motion
The early goal is pain modulation and preventing the patient from locking into a guarded, immobile posture. Treatment is gentle: manual therapy to reduce muscle spasm, pain-modulated cervical range-of-motion work, scapular and postural cueing, and short, frequent activity bouts at home. Soft cervical collars are not used for typical WAD I–II — prolonged immobilization is associated with worse outcomes.
Week 2–6: active rehabilitation
As pain settles, treatment shifts to active rehabilitation — strengthening the deep cervical flexors, retraining scapular stabilizers, restoring full cervical and thoracic range of motion, and addressing any vestibular or oculomotor symptoms. Patients often feel substantially better in this window even though full functional recovery is still ahead.
Week 6–12: functional return
Treatment in this phase is built around the patient's actual life — return to driving, return to desk work, lifting their child, sleeping through the night. Frequency tapers, the home exercise program expands, and the chart should show measurable functional progress at each reassessment.
Beyond 12 weeks: chronic WAD
A smaller share of patients — meaningful, but a minority — develop persistent symptoms past three months. This is chronic whiplash-associated disorder. More imaging usually doesn't help. What does help is a structured, graded rehabilitation program with pain-science education, progressive loading, and management of any vestibular or cognitive symptoms.
What the evidence says about treatment
The clinical literature consistently favors early, active treatment over rest or passive modalities alone. Patients who begin guided rehabilitation within the first 1–3 weeks return to function faster and report lower pain scores at 6 months than patients who wait. The U.S. Centers for Disease Control and Prevention and the American College of Physicians both recommend non-drug treatments such as physical therapy as a first-line option for musculoskeletal and chronic pain.
Across post-injury populations more broadly, the early-PT evidence is striking. A 2018 Stanford and Duke study published in JAMA Network Open (88,985 patients) found that people who started physical therapy soon after a diagnosis of shoulder, neck, low-back, or knee pain were about 7–16% less likely to use opioids in the following months. Research on early PT after emergency-department visits for low-back pain has also linked early PT with lower risk of lumbar surgery, lower likelihood of long-term opioid use, and lower overall costs.
Why in-home PT fits whiplash care
Whiplash is the injury most likely to make a patient afraid to drive. We see this every week — patients who logically know they should attend PT but cannot bring themselves to get into a car. In-home delivery removes that barrier entirely. Treatment starts in the living room, with the therapist guiding cervical motion, postural retraining, and graded exposure to activity without the patient ever having to be a passenger.
It also lets the therapist work on the actual surfaces and activities that matter — the patient's own bed, their car, the chair at their desk — instead of generic clinic equipment.
Frequently asked questions
- Why didn't my neck hurt at the scene of the crash?
- Whiplash symptoms commonly peak 24 to 72 hours after the crash as inflammation develops and adrenaline wears off. Feeling fine at the scene is not evidence you weren't injured. Get evaluated by a qualifying provider within 14 days regardless.
- Do I need an MRI?
- Most WAD I–II cases don't require an MRI. Imaging is indicated when there are neurological signs, suspected fracture, or symptoms that fail to improve as expected. Your treating provider will decide based on the clinical exam.
- Should I wear a cervical collar?
- For typical whiplash without fracture or instability, prolonged use of a soft cervical collar is associated with worse outcomes, not better. Active, graded motion is the recommended approach.
- How long until I can drive again?
- Most WAD I–II patients return to driving within 2 to 4 weeks. The decision is functional — adequate cervical rotation to shoulder-check, no symptoms that meaningfully impair attention, and the patient's own confidence to operate the vehicle safely. Your PT will help assess this.
Related articles
- Recovering After a Crash
How Soon Should You Start PT After a Car Accident in Florida?
In Florida, the practical answer is within 14 days — both because the PIP statute requires initial care in that window and because the clinical evidence strongly favors early intervention for soft-tissue and cervical-spine injuries.
Andre Bennett, PT, DPT · May 2, 2026
- Florida PIP & MedPay
Does Florida PIP Cover Physical Therapy After a Car Accident?
Yes — Florida Personal Injury Protection (PIP) covers medically necessary physical therapy after a car accident, but only if the patient is first evaluated by a qualifying provider within 14 days of the crash. Here's what that means in practice.
Dr. Sam Rose, PT, DPT · March 4, 2026
- In-Home PT
Why Auto-Accident Patients Skip PT — and How In-Home Care Fixes It
Roughly half of patients referred to outpatient physical therapy after a car accident never complete the prescribed plan of care. The reasons are mostly logistical, not medical — which is why moving treatment into the home dramatically improves attendance.
Dr. Sam Rose, PT, DPT · April 8, 2026
In your city
Conditions we treat across Florida
Each city page below covers the clinical evidence, recovery timelines, and PIP details specific to these conditions.
- Whiplash — Tampa
- Whiplash — Orlando
- Whiplash — Miami
- Whiplash — St. Petersburg
- Concussion — Tampa
- Concussion — Orlando
- Concussion — Miami
- Concussion — St. Petersburg
Don’t see your city? View all Florida service areas.
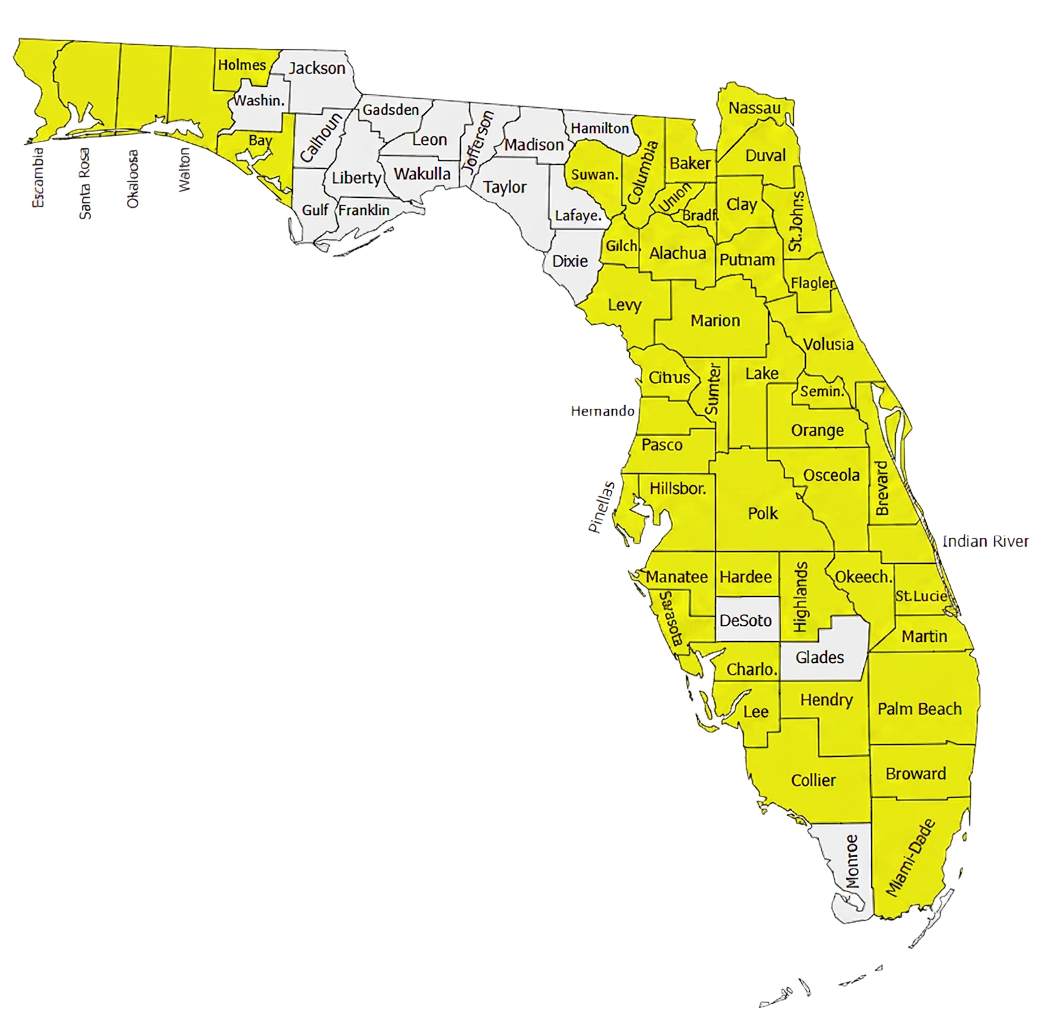
500+ Physical Therapists covering 35+ counties in Florida.
Our clinician network reaches major metros and rural communities alike — from the Panhandle to the Keys. If a patient is in a highlighted county, we can usually see them at home within 24–72 hours of intake.
- Clinicians in network
- 500+
- Florida counties covered
- 35+
Need to refer a Florida patient?
Our intake team confirms PIP and MedPay coverage during the call and schedules most patients for an in-home evaluation within 48 hours.