The Ultimate Physical Therapy Cheat Sheet for Patients and Clinicians
A practical reference for how good PT works: evaluation, SOAP notes, SMART goals, common modalities, and the documentation patients have every right to ask for.
Dr. Sam Rose, PT, DPT
Clinical Director, PT Near Me
Examination versus evaluation — the difference matters
On your first physical therapy visit, the clinician does two related but distinct things. The examination is data collection: history, observation, range of motion measurements, manual muscle testing, palpation, special tests, and functional tests like the Lower Extremity Functional Scale (LEFS) or the Disabilities of the Arm, Shoulder and Hand (DASH). It produces numbers and observations.
The evaluation is the interpretation of that data. It's the clinical reasoning that turns numbers into a movement diagnosis, a prognosis, and a plan of care. CPT codes 97161, 97162, and 97163 reflect the complexity of the evaluation — low, moderate, or high — based on the number of body systems involved, the comorbidities, and the clinical decision-making required.
| Examination | Evaluation |
|---|---|
| Data collection | Data interpretation |
| History, ROM, MMT, special tests | Movement diagnosis, prognosis, plan of care |
| Numbers and observations | Clinical reasoning |
| Repeated at re-eval points to measure change | Updated when the picture changes |
If a clinician hands you a plan of care without first doing a thorough examination, that's a quality issue worth raising. The plan should be the conclusion of the reasoning, not its starting point.
The SOAP note — the standard for every visit
Every treatment visit should produce a SOAP note. SOAP stands for Subjective, Objective, Assessment, and Plan, and it's the format physicians, therapists, and payers expect.
Subjective
What the patient reports. "Pt reports neck pain rated 5/10 at rest, 8/10 with right rotation. Sleep disturbed 2 of 7 nights this week." Quote the patient when possible; use measurable scales (numeric pain rating, sleep nights affected, hours sitting before symptom onset) so progress can be tracked.
Objective
What the therapist measured or observed. Range of motion, manual muscle test grades, gait deviations, balance scores, special test findings, and the interventions performed in the session (with time and dose). "Cervical AROM right rotation 45° (was 30° on eval). MMT deep neck flexors 3/5. Performed manual therapy to upper cervical spine, 15 min therapeutic exercise to deep neck flexors and scapular stabilizers."
Assessment
The clinical interpretation. Is the patient improving, plateauing, or worsening? How does today connect to the goals? "Pt continues to make steady gains in cervical AROM and is meeting short-term goal of 50% improvement in rotation. Tolerating progression of resistive exercises without symptom flare. Continue current plan."
Plan
What's next. Frequency, duration, interventions, and progressions. Updates to the home exercise program. Coordination with the referring physician or surgeon. "Continue 2x/week for 4 more weeks. Progress to thoracic mobility and dynamic stabilization next visit. Home program updated; copy sent to patient."
SMART goals: how good plans of care set targets
Vague goals are useless. "Improve strength" or "reduce pain" can't be measured, which means they can't be achieved or appealed. SMART goals — Specific, Measurable, Achievable, Relevant, Time-bound — are how clinicians turn intent into something a patient and a payer can track.
- Weak: "Improve shoulder ROM."
- SMART: "Increase right shoulder flexion AROM from 110° to 160° within 6 weeks to allow overhead reaching for upper-shelf tasks at home."
- Weak: "Walk better."
- SMART: "Ambulate 200 feet without an assistive device and without loss of balance within 4 weeks, to return to grocery shopping independently."
- Weak: "Reduce pain."
- SMART: "Decrease low back pain from 6/10 to 3/10 on the numeric pain rating scale during sitting tolerance > 30 minutes within 4 weeks."
Goals should be tied to function the patient cares about — getting back to work, walking the dog, sleeping through the night, driving — not abstract metrics. The numbers exist to prove the function is returning.
Common interventions and modalities
The toolbox is large; here are the categories you'll see most often on a Florida PT visit.
| Intervention | What it does |
|---|---|
| Therapeutic exercise (TheraEx) | Strength, endurance, flexibility — the backbone of every plan |
| Manual therapy | Hands-on joint mobilization and soft-tissue work to restore motion and reduce guarding |
| Neuromuscular re-education (NMR) | Retraining movement patterns, postural control, and proprioception |
| Gait training | Restoring a safe, efficient walking pattern with or without an assistive device |
| Therapeutic activities | Task-specific functional retraining — transfers, lifting, reaching |
| Electrical stimulation (e-stim) | Pain modulation, muscle re-education; used selectively, not as a standalone plan |
| Therapeutic ultrasound | Deep heating of soft tissue; evidence is mixed and use is selective |
| Cryotherapy / heat | Symptom management; an adjunct, not a treatment in itself |
A red flag worth knowing: if every visit is mostly passive modalities — hot pack, ultrasound, e-stim — with little active exercise or hands-on work, the plan is probably under-dosed. Active interventions drive recovery; passive ones manage symptoms.
Common documentation problems patients should know about
- Copy-pasted notes that look identical session after session — your status changes daily, the note should reflect that.
- Vague language like "tolerated treatment well" without functional benchmarks.
- Missing time documentation when CPT codes require it (97110 therapeutic exercise is billed in 15-minute increments and the note has to support the units).
- Goals that never get re-measured. A goal at week one that's still sitting un-scored at week eight tells you no one is tracking.
- Discharge with no summary. Every episode of care ends with a discharge note; you should be able to request a copy.
What patients have a right to ask for
You are entitled to the records of your own care. Under HIPAA, you can request a copy of your initial evaluation, your progress notes, your re-evaluations, and your discharge summary. This matters in three situations especially: when a treating physician asks for an update, when an auto-insurance adjuster requests records to support a PIP claim, and when you're transitioning to a different provider.
A practice that's slow or evasive about producing documentation is one to question. Good clinicians are proud of their notes because the notes show the work.
Frameworks therapists use behind the scenes
Good evaluations don't happen by intuition. Experienced clinicians lean on frameworks that force them to look at a presentation from multiple angles, then synthesize. A few that drive the decisions you'll see in your plan.
SINSS
Severity, Irritability, Nature, Stage, Stability. SINSS describes how active and reactive a problem is. A highly severe and irritable presentation (think: a fresh whiplash where any movement spikes pain for an hour) calls for a very different early plan than a chronic, low-irritability presentation. Reading SINSS in the eval determines dose, frequency, and how aggressive the early program can be.
ICF model
The International Classification of Functioning, Disability and Health asks the clinician to consider three levels at the same time: body structure and function (joint, muscle, tissue), activity (what tasks the patient can do), and participation (the roles in life — work, family, recreation — the patient wants back). A plan that only addresses the joint without driving toward participation is incomplete.
Movement system diagnosis
Rather than naming a structural diagnosis ("rotator cuff tendinopathy"), movement system diagnosis names the underlying movement impairment ("scapular downward rotation syndrome with insufficient serratus activation"). This matters because two patients with the same MRI can have very different movement problems — and therefore very different plans.
Standardized outcome measures patients should expect to see
Numbers prove progress. A good plan of care will use one or more validated outcome measures appropriate to the body region and the patient's function. These get scored on the eval and re-scored at intervals so the trend is visible.
| Body region | Outcome measure |
|---|---|
| Lower extremity / general mobility | Lower Extremity Functional Scale (LEFS) |
| Upper extremity | Disabilities of the Arm, Shoulder and Hand (DASH or QuickDASH) |
| Neck | Neck Disability Index (NDI) |
| Low back | Oswestry Disability Index (ODI), Modified Oswestry |
| Knee | Knee Outcome Survey, KOOS |
| Shoulder | SPADI, ASES |
| Balance / falls risk | Berg Balance Scale, Timed Up and Go (TUG), 5x Sit-to-Stand |
| Concussion / vestibular | VOMS, Dynamic Gait Index |
If your evaluation didn't include any standardized measure, ask. They're free, take a few minutes, and they give you and the referring physician a real number to track. Without them, "feeling better" is the only progress signal — and that's not enough for a plan that may extend across many weeks.
How PT Near Me documents care
Every plan of care is signed by the evaluating Doctor of Physical Therapy. Re-evaluations occur on the schedule required by Florida practice rules and payer policy, and goals are scored, not just listed. If a goal isn't progressing, we change the plan; we don't keep doing the same thing.
Documentation is also where coordination with the referring office happens. The initial evaluation, every progress re-evaluation, and the discharge summary are sent back so the treating physician sees the same picture we do — not a generic confirmation that PT happened, but the actual measurements, the goals scored against, and what changed in the plan. For post-MVA cases this matters because the chart is going to be read by the PIP carrier later, and gaps or vague language at the PT level become problems down the line. Clean documentation up front keeps the record clean throughout.
Patients can request their own records at any time and we send them at no charge. We encourage it. The best advocate for your own recovery is a patient who has read their own evaluation and knows what the goals are.
Related reading
Frequently asked questions
- Can I get a copy of my PT notes?
- Yes. Under HIPAA you have the right to access your own records, including the initial evaluation, progress notes, and discharge summary. We provide them at no charge.
- How often should my plan of care be re-evaluated?
- Florida practice rules and most payers require formal re-evaluation at set intervals — typically every 30 days or after a defined number of visits, whichever comes first. Informal progression decisions happen every visit.
- What does CPT code 97110 mean on my bill?
- 97110 is therapeutic exercise, billed in 15-minute increments. The note should show what exercises were performed and roughly how long, so the units match the documentation.
- Is it normal for PT to use ultrasound or e-stim every visit?
- Selective use is fine; routine reliance is a warning sign. The bulk of any plan should be active — exercise, manual therapy, neuromuscular re-education — because that's what drives recovery.
- What happens at discharge?
- You get a discharge summary documenting where you started, where you ended, which goals were met, and any remaining recommendations including the final home exercise program. A copy goes to the referring physician.
- Should my home exercise program change over time?
- Yes. A program that doesn't progress is a sign no one is paying attention. Expect updates every two to three weeks — different exercises, more resistance, harder variations — to keep pace with what your body can handle.
Related articles
- PT Basics & Glossary
Physical Therapy Terminology: A Plain-English Guide to PT Lingo
A patient-friendly guide to the words, abbreviations, and movement terms physical therapists use every day — so you can follow your plan of care and ask better questions.
Dr. Sam Rose, PT, DPT · June 22, 2026
- PT Basics & Glossary
Physical Therapist vs. PTA: Roles, Education, and Differences
PTs and PTAs both treat patients, but they aren't interchangeable. A clear look at scope, education, and what each role does during your care.
Dr. Sam Rose, PT, DPT · June 22, 2026
- For Physicians
A Physician's Guide to Post-Discharge In-Home PT in Florida
When a Florida auto-accident patient leaves your ER or post-op visit with a PT referral, the single biggest determinant of whether they actually complete care is whether the therapy is accessible. In-home PT closes the post-discharge attendance gap and returns clinic-equivalent documentation to your office.
Dr. Maria Alvarez, PT, DPT · June 22, 2026
In your city
Conditions we treat across Florida
Each city page below covers the clinical evidence, recovery timelines, and PIP details specific to these conditions.
- Whiplash — Tampa
- Whiplash — Orlando
- Whiplash — Miami
- Whiplash — St. Petersburg
- Low Back Pain — Tampa
- Low Back Pain — Orlando
- Low Back Pain — Miami
- Low Back Pain — St. Petersburg
- Concussion — Tampa
- Concussion — Orlando
- Concussion — Miami
- Concussion — St. Petersburg
- Shoulder Injury — Tampa
- Shoulder Injury — Orlando
- Shoulder Injury — Miami
- Shoulder Injury — St. Petersburg
Don’t see your city? View all Florida service areas.
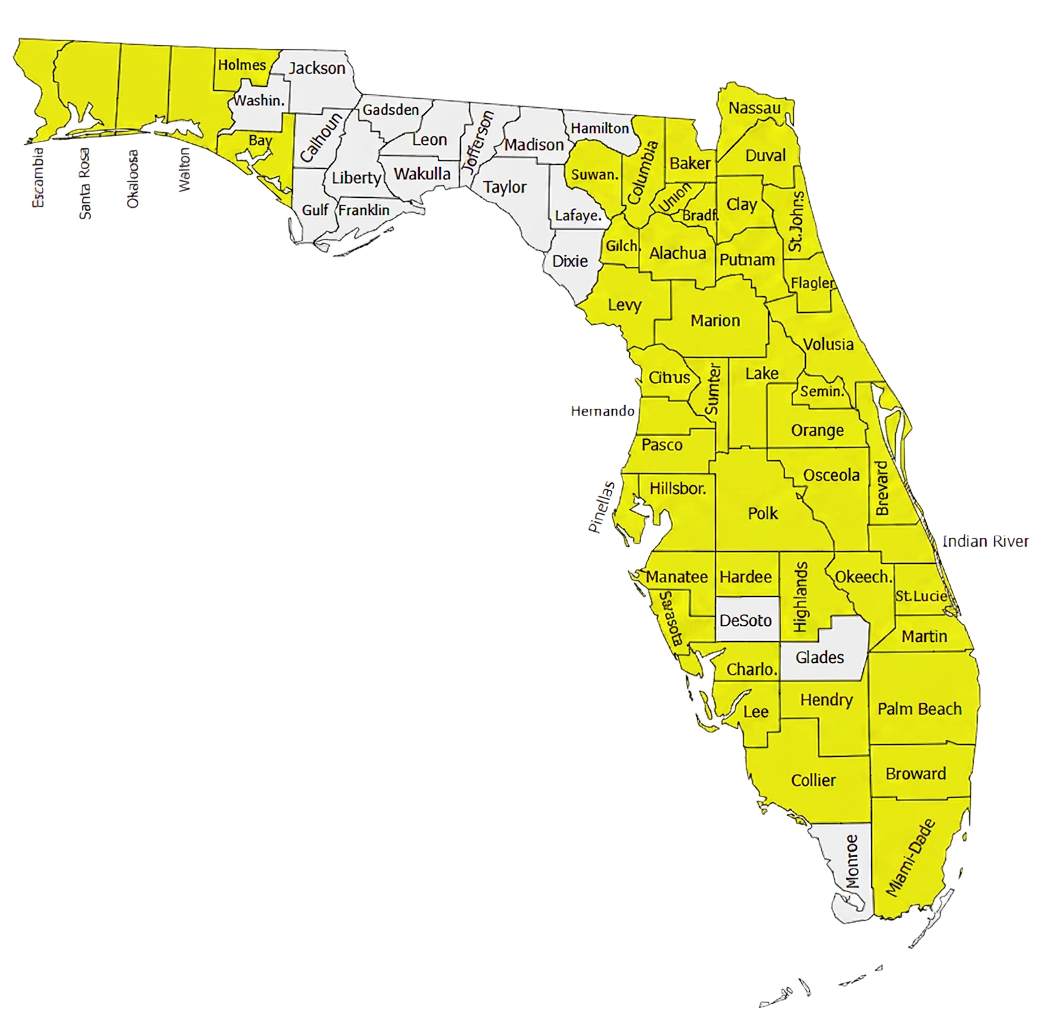
500+ Physical Therapists covering 35+ counties in Florida.
Our clinician network reaches major metros and rural communities alike — from the Panhandle to the Keys. If a patient is in a highlighted county, we can usually see them at home within 24–72 hours of intake.
- Clinicians in network
- 500+
- Florida counties covered
- 35+
Need to refer a Florida patient?
Our intake team confirms PIP and MedPay coverage during the call and schedules most patients for an in-home evaluation within 48 hours.