Mobile Physical Therapy: The In-Home PT Guide for Florida Patients
How mobile, in-home physical therapy actually works in Florida — from referral and first visit to discharge — and when it's the right level of care.
Dr. Sam Rose, PT, DPT
Clinical Director, PT Near Me
What in-home, mobile physical therapy actually is
Mobile physical therapy is exactly what it sounds like: the therapist comes to the patient. Same licensure, same scope of practice, same documentation standards as clinic-based PT — different setting. In Florida the model has grown quickly because it solves problems clinic PT has always struggled with: scheduling friction, transportation barriers, no-shows after a crash or surgery, and home environments the therapist never gets to see.
At PT Near Me, every patient is evaluated and treated by a Florida-licensed Doctor of Physical Therapy. We staff 500+ clinicians across 35+ Florida counties, which means most referrals can be matched to a therapist who lives in or near the patient's community. The first visit is typically within 48 hours of the referral, and we work afterhours and weekends when the case calls for it.
Who in-home PT is the right fit for
- Auto-accident patients in the first 14 days, when Florida PIP requires you to receive initial services and care to preserve full benefits.
- Post-surgical patients (joint replacement, rotator cuff, spine, ACL) who don't yet drive and whose first weeks are spent on stairs, transfers, and ADLs at home.
- Older adults recovering from a fall, a hospitalization, or a deconditioning episode — in-home care lets us train balance and transfers in the actual living room, kitchen, and bathroom.
- Patients with chronic pain or mobility limitations for whom getting in and out of a car repeatedly is itself a barrier to consistent treatment.
- Patients who simply can't reliably get to a clinic three times a week — caregivers, parents of small children, and shift workers.
It's not the right setting for everything. Some specialized equipment lives in a clinic. Some patients are at a stage where progressing under heavy load in a gym is the most efficient path. A good intake conversation sorts this out before the first visit, and we'll say so if clinic-based care is a better match for a given case.
What happens on the first visit
The first visit is a full evaluation. The therapist arrives with intake documents prepared from your referral and any imaging or surgical paperwork already in our records. The visit typically runs 60 to 75 minutes and covers four things.
- Subjective history: how the injury or surgery happened, what hurts, what's hard, what your day looks like, what your goals are.
- Objective examination: range of motion, manual muscle testing, special tests relevant to the body region, gait if applicable, and a functional assessment in your actual home environment.
- Clinical reasoning and plan of care: movement diagnosis, prognosis, short- and long-term goals, frequency, duration, and the interventions that will be used.
- First treatment and home exercise program: we don't wait until visit two to start. You get hands-on work that day, you get the initial home program written down with photos or videos, and we coordinate the second visit before we leave.
The evaluation note goes back to the referring physician within 24–48 hours, so the patient and the referring office are on the same page from day one.
What a treatment session looks like
Sessions are typically 45 to 60 minutes. The therapist arrives with portable equipment — resistance bands, weights, a portable treatment table when needed, balance equipment, and basic modality tools. The session usually combines four elements.
- Hands-on manual therapy to the body region driving the symptoms — joint mobilization, soft-tissue work, neural mobilization as indicated.
- Therapeutic exercise progressed from the prior session, dosed in sets and reps with a clear target (strength, motor control, endurance, or capacity).
- Functional retraining specific to your environment: stair training on your actual stairs, transfer training in your actual bathroom, gait training in your actual hallway.
- Home program review and progression. We don't hand out generic sheets; the program changes as you progress, and we make sure you can actually do every exercise before we leave.
Why the home environment matters clinically
A patient who walks beautifully across a clinic floor and then trips at home isn't a clinic problem. They're an environment problem. In-home PT lets us train the exact transfers, the exact stairs, and the exact reaching tasks the patient does every day. We see the rug edges, the bathroom layout, the bed height, the chair the patient actually sits in for hours, and we build the program around those things.
For post-MVA patients, the home environment also drives compliance. The auto-accident population is one of the highest no-show populations in outpatient PT — pain, schedule disruption, transportation, fatigue, and the cognitive load of dealing with the crash all stack up. Removing the trip to the clinic removes the biggest reason people drop out of care before they finish their plan.
How billing works for Florida auto-accident patients
For motor vehicle accident cases, PT Near Me bills Florida Personal Injury Protection (PIP) first. PIP is required on every Florida auto policy and covers 80% of reasonable and necessary medical expenses up to the $10,000 limit, when initial services and care are received within 14 days of the crash. After the deductible and 80% are accounted for, the remaining 20% is typically picked up by MedPay if the patient's auto policy includes it.
Common conditions we treat at home
- Post-MVA orthopedic injury: cervical strain (whiplash), thoracic and lumbar sprain, shoulder and knee injuries from seatbelt and impact forces, concussion-related vestibular issues.
- Post-surgical rehab: total knee and hip replacement, rotator cuff repair, ACL reconstruction, lumbar fusion and discectomy, ankle ORIF.
- Fall recovery and deconditioning in older adults, including balance retraining and home safety adjustments.
- Chronic neck, low back, and joint pain where access to consistent care has been the limiting factor.
- Generalized weakness after hospitalization for non-orthopedic causes (pneumonia, cardiac events) where home-based reconditioning is appropriate.
In-home PT vs. clinic PT vs. Medicare home health
"PT at home" can mean three different things, and people mix them up. The differences matter for what you're billed and what's allowed.
Clinic-based outpatient PT
You drive to a clinic. The clinic owns specialized equipment, the schedule is fixed, and you fit your day around the appointment. This is the default model and the right answer for some cases — high-load strength training, sport-specific return-to-play, or anything that genuinely needs equipment that doesn't travel.
Mobile / in-home outpatient PT (what we do)
A Doctor of Physical Therapy comes to your home and delivers outpatient PT in your environment. Same scope of practice as clinic PT, same documentation, same plan of care. No homebound requirement, no episode-of-care framework. For Florida auto-accident patients this is billed PIP first, then MedPay if the auto policy includes it.
Medicare home health
A specific Medicare benefit for patients certified as homebound by a physician. It's an interdisciplinary episode-of-care framework (nursing, PT, OT, home health aide) billed under Part A. It is not the right benefit for a Florida auto-accident case because the injury is auto-related and PIP is the primary payer. Running an auto-accident through home health distorts the clinical record and complicates the payer picture.
What to expect physically over the first 6 weeks
Recovery is rarely linear. Patients who know what a normal arc looks like are less likely to panic at a setback and more likely to stay with the plan long enough to actually finish.
- Week 1–2: Symptom modulation. The focus is reducing pain irritability, restoring early motion, and protecting healing tissue. Expect tenderness, fatigue after sessions, and a home program built around frequent short bouts rather than long workouts.
- Week 2–4: Active loading. Gentle progressive loading begins. You should start to see range of motion measurable change and pain numbers trending down. Soreness after exercise is normal; sharp pain that lingers is not.
- Week 4–6: Strength and capacity. Loading progresses to meaningful resistance. Functional benchmarks — sitting tolerance, walking distance, stairs, lifting capacity — become the primary goals. The home program gets harder, not easier.
- Week 6 and beyond: Return to function. The plan focuses on whatever you wanted back — work, driving, sport, sleep. Discharge happens when goals are met or when progress has clearly plateaued and you can self-manage with a continuing home program.
How to get started
Most referrals come from primary care, orthopedics, neurology, physiatry, and hospital discharge planners. Patients can also self-refer for an evaluation after an auto accident. Intake takes a few minutes by phone, fax, or our online referral form, and the first visit is usually within 48 hours.
Before the first visit, our intake team confirms the auto policy, verifies the 14-day PIP timing window, gathers any imaging or surgical paperwork from the referring office, and matches the case with a therapist who lives in or near the patient's area. The patient gets a confirmation with the therapist's name, arrival window, and what to have ready — nothing complicated, just enough to make the first 60 minutes productive.
Related reading
Frequently asked questions
- How quickly can the first visit be scheduled?
- Typically within 48 hours of referral. For post-MVA cases inside the Florida 14-day window we prioritize same-week scheduling so the initial-services requirement is met.
- Do I need a physician referral?
- Florida allows direct access to physical therapy for evaluation, and many patients start that way after a crash. For ongoing care under PIP we coordinate with the treating physician on record.
- Will the same therapist see me every visit?
- Continuity is the goal. Most patients see the same primary Doctor of Physical Therapy through their episode of care.
- What if my home doesn't have enough space?
- We've treated patients in studio apartments, assisted living rooms, and second-floor walk-ups. Most therapeutic exercise needs less floor space than people expect, and the realism is part of the point — your program should work in the space you live in.
- Do you bill my health insurance?
- No. PT Near Me bills Florida PIP first and MedPay if the auto policy includes it. We do not bill commercial health insurance.
- What areas of Florida do you cover?
- 47 cities across Tampa Bay, Central Florida, South Florida, and North Florida, with 35+ counties served. See the full list on the Service Areas page.
- What should I have ready for the first visit?
- Your auto-policy declarations page if you have it, any ER discharge paperwork or imaging from the crash, a list of medications, and a space with room for the therapist to set up — kitchen table or living room floor is fine.
Related articles
- In-Home PT
Why Auto-Accident Patients Skip PT — and How In-Home Care Fixes It
Roughly half of patients referred to outpatient physical therapy after a car accident never complete the prescribed plan of care. The reasons are mostly logistical, not medical — which is why moving treatment into the home dramatically improves attendance.
Dr. Sam Rose, PT, DPT · April 8, 2026
- Recovering After a Crash
How Soon Should You Start PT After a Car Accident in Florida?
In Florida, the practical answer is within 14 days — both because the PIP statute requires initial care in that window and because the clinical evidence strongly favors early intervention for soft-tissue and cervical-spine injuries.
Andre Bennett, PT, DPT · May 2, 2026
- In-Home PT
In-Home PT vs. Medicare Home Health: What's the Difference?
In-home physical therapy and Medicare home health both send a clinician to the patient's house, but they're regulated, billed, and clinically scoped very differently. After a Florida car accident, in-home PT is almost always the right fit — Medicare home health usually isn't an option at all.
Dr. Maria Alvarez, PT, DPT · June 22, 2026
In your city
Conditions we treat across Florida
Each city page below covers the clinical evidence, recovery timelines, and PIP details specific to these conditions.
- Low Back Pain — Tampa
- Low Back Pain — Orlando
- Low Back Pain — Miami
- Low Back Pain — St. Petersburg
- Shoulder Injury — Tampa
- Shoulder Injury — Orlando
- Shoulder Injury — Miami
- Shoulder Injury — St. Petersburg
- Knee Injury — Tampa
- Knee Injury — Orlando
- Knee Injury — Miami
- Knee Injury — St. Petersburg
- Herniated Disc — Tampa
- Herniated Disc — Orlando
- Herniated Disc — Miami
- Herniated Disc — St. Petersburg
- Post-Fracture Rehab — Tampa
- Post-Fracture Rehab — Orlando
- Post-Fracture Rehab — Miami
- Post-Fracture Rehab — St. Petersburg
- Post-Surgical Rehab — Tampa
- Post-Surgical Rehab — Orlando
- Post-Surgical Rehab — Miami
- Post-Surgical Rehab — St. Petersburg
Don’t see your city? View all Florida service areas.
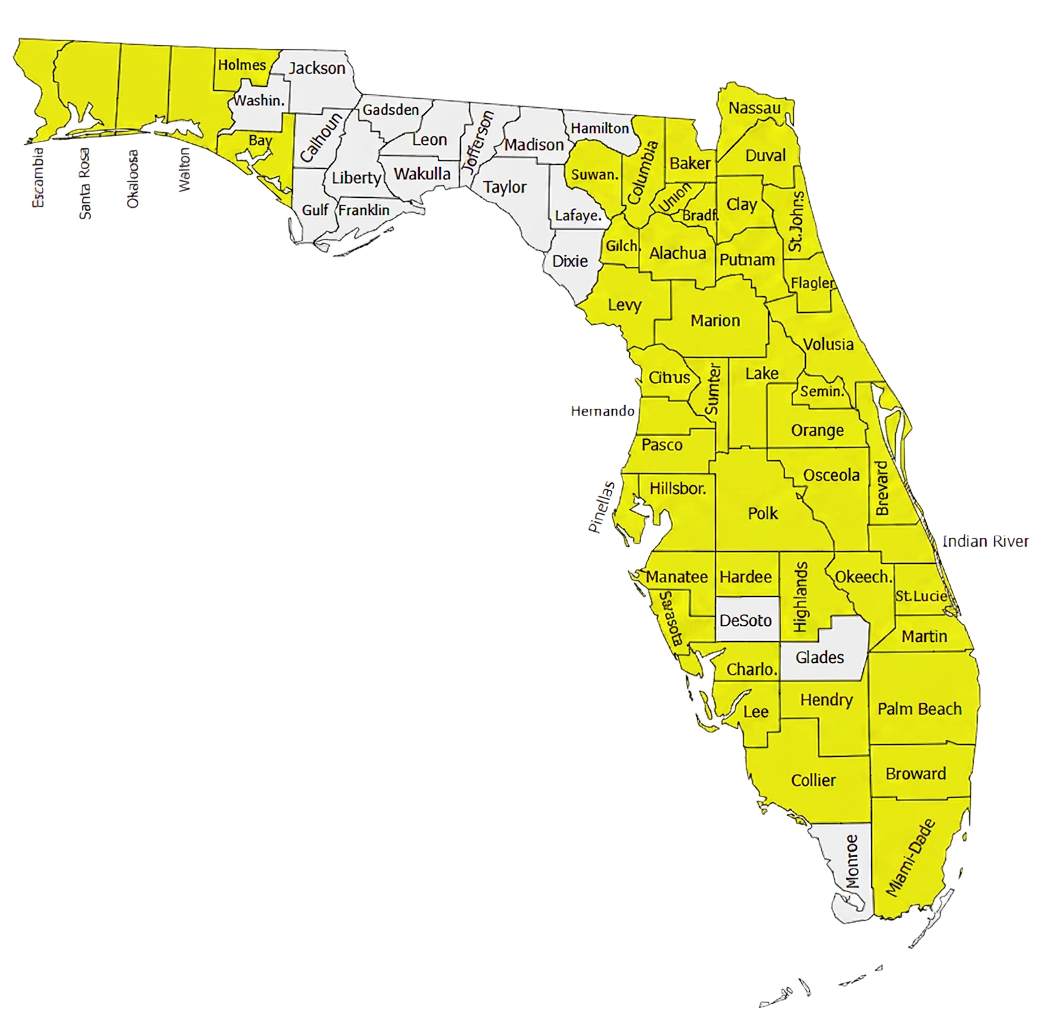
500+ Physical Therapists covering 35+ counties in Florida.
Our clinician network reaches major metros and rural communities alike — from the Panhandle to the Keys. If a patient is in a highlighted county, we can usually see them at home within 24–72 hours of intake.
- Clinicians in network
- 500+
- Florida counties covered
- 35+
Need to refer a Florida patient?
Our intake team confirms PIP and MedPay coverage during the call and schedules most patients for an in-home evaluation within 48 hours.