Documenting Pain After a Car Accident: Scales & PIP Records
Consistent pain and functional documentation is what turns a recovery into a defensible PIP medical record — and what gives your physician the data to manage care. Here is how the 0–10 and VAS pain scales work, what PT progress notes capture, and why it matters in Florida.
Dr. Sam Rose, PT, DPT
Clinical Director, PT Near Me
Why pain documentation matters after a crash
Florida PIP pays for care that is medically necessary, and 'medically necessary' is judged on the clinical record. The clearer the record of pain levels, functional limitations, and response to treatment, the less friction the patient and provider face when PIP reviews the case. Documentation also lets the referring physician see whether the plan of care is working, and lets a future treating clinician understand the recovery arc — exactly the continuity-of-care problem PT progress notes are designed to solve.
Federal guidance from agencies like the CDC repeatedly emphasizes that pain assessment should combine self-reported intensity with functional measures rather than rely on a single number in isolation. That principle drives how a good PT note is structured.
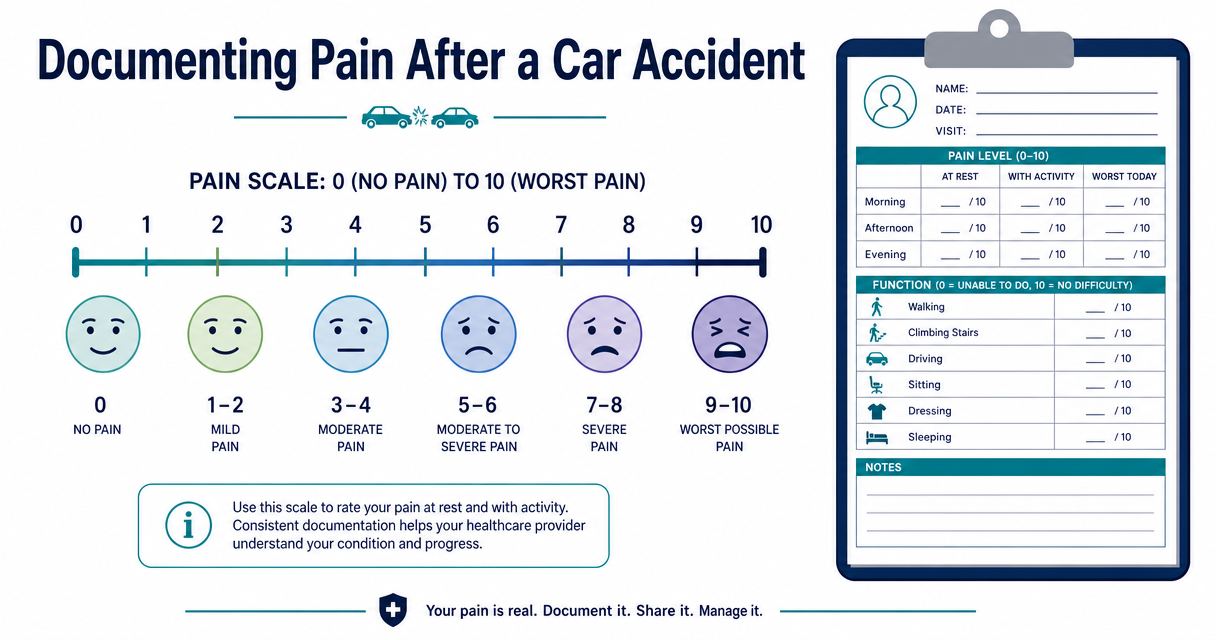
The two pain scales most providers use
| Scale | How it works | Best used for |
|---|---|---|
| Numeric Pain Rating Scale (NPRS, 0–10) | Patient picks a number between 0 (no pain) and 10 (worst imaginable pain) | Quick, repeatable visit-by-visit check |
| Visual Analog Scale (VAS) | Patient marks a point on a 100mm line from no pain to worst possible pain | More granular research- and chronic-pain settings |
| Faces Pain Scale (revised) | Cartoon faces, no numbers | Pediatrics or patients with language barriers |
| Pain interference questions | How much did pain interfere with sleep / work / daily activities (0–10)? | Capturing functional impact, not just intensity |
A clinically useful note rarely uses just one of these. The standard post-MVA PT documentation captures NPRS at rest, NPRS with activity, and at least one pain-interference question (e.g., 'how much did pain interfere with sleep last night?') at every visit. Trending all three matters more than the absolute number on any one visit.
What a PT evaluation and progress note actually capture
- Subjective: patient-reported symptoms, NPRS at rest and with activity, sleep, function (work, driving, household tasks), and any change since the last visit.
- Objective: range of motion in degrees, manual muscle test grades, special tests, gait observations, and standardized outcome measures (e.g., the Neck Disability Index for cervical cases or the Oswestry for the lumbar spine).
- Assessment: the therapist's clinical reasoning — what is driving today's presentation, how it compares to the prior visit, whether progress is on track.
- Plan: what was treated today, what changed in the plan of care, what the patient is doing for the home exercise program, when the next visit is scheduled.
Across an episode of care that pattern produces a longitudinal record showing exactly what changed, when, and why. That is the form of documentation PIP reviewers, physicians, and case managers can act on.
Why pain alone is not enough
A patient who reports 7/10 pain with 90 degrees of shoulder flexion at week two and 7/10 pain with 150 degrees of flexion at week six is making real progress, even though the pain number did not move. A patient who reports 3/10 pain but cannot lift a gallon of milk to a shelf is still impaired. Pain numbers paired with functional measures tell the story; pain numbers alone do not.
This is why every visit pairs a pain rating with at least one functional metric — range of motion, single-leg balance time, sit-to-stand reps in 30 seconds, distance walked, or a standardized outcome score. The combination is what makes the record meaningful.
How in-home PT documents care
In-home physical therapy uses the same EMR, the same CPT codes, and the same clinical documentation standards as a clinic. The therapist arrives with a tablet or laptop, records the visit at the bedside, and the note routes to the referring physician on the standard reporting cadence — evaluation within 24–48 hours of the first visit, progress notes every two weeks, a re-evaluation at 30 days, and a discharge summary at the end of the episode of care. See For Physicians for the full SLA.
For patients who want to do their part, keeping a brief daily symptom log (NPRS at rest and with activity, sleep hours, what they did) gives the therapist higher-resolution data to work with. We give patients a printable log on the first visit.
Documentation and Florida PIP
Florida PIP reimburses medically necessary care, and medical necessity is established in the clinical record. The 14-day rule — see our 14-day rule explainer — sets the deadline for the first qualifying visit, and the documentation produced from that first visit forward is what supports continued treatment. Good notes are not optional and they are not just for the PT; they are the practical evidence base for the entire plan of care.
For a glossary of the documentation terms used here (NPRS, ROM, MMT, HEP, POC), see the PT Near Me glossary. For the full PIP coverage picture, see does Florida PIP cover physical therapy.
Frequently asked questions
- What is the difference between the NPRS and the VAS pain scales?
- The NPRS asks the patient to pick a number from 0 to 10. The VAS asks the patient to mark a point on a 100mm line. Both measure pain intensity; the VAS is more granular and is more common in research, while the NPRS is more common in busy clinical settings.
- How often should I rate my pain after a car accident?
- At minimum at every clinical visit. Many patients benefit from a brief daily log — pain at rest, pain with activity, sleep, and what they did that day — which gives the PT and the referring physician higher-resolution data than memory alone.
- Does PT documentation count for Florida PIP medical necessity?
- Yes. PT evaluations, daily notes, re-evaluations, and discharge summaries are part of the medical record that supports PIP medical necessity. The notes use standardized formats and the same coding used in any outpatient clinic.
- Is in-home PT documentation as thorough as clinic-based PT documentation?
- Yes. PT Near Me clinicians use the same EMR, the same CPT codes, and the same documentation standards as a clinic-based PT. The notes route to the referring physician on a defined cadence.
Related articles
- Florida PIP & MedPay
Does Florida PIP Cover Physical Therapy After a Car Accident?
Yes — Florida Personal Injury Protection (PIP) covers medically necessary physical therapy after a car accident, but only if the patient is first evaluated by a qualifying provider within 14 days of the crash. Here's what that means in practice.
Dr. Sam Rose, PT, DPT · March 4, 2026
- Florida PIP & MedPay
The Florida 14-Day Rule: Why You Must Start Treatment Fast
Florida's 14-day rule says an injured driver, passenger, or pedestrian must receive initial medical care within 14 days of a crash, or PIP benefits are forfeited entirely. Here's exactly what counts, who can provide that care, and what happens if the window closes.
Dr. Sam Rose, PT, DPT · June 20, 2026
- In-Home PT
Why Auto-Accident Patients Skip PT — and How In-Home Care Fixes It
Roughly half of patients referred to outpatient physical therapy after a car accident never complete the prescribed plan of care. The reasons are mostly logistical, not medical — which is why moving treatment into the home dramatically improves attendance.
Dr. Sam Rose, PT, DPT · April 8, 2026
In your city
Conditions we treat across Florida
Each city page below covers the clinical evidence, recovery timelines, and PIP details specific to these conditions.
- Whiplash — Tampa
- Whiplash — Orlando
- Whiplash — Miami
- Whiplash — St. Petersburg
- Low Back Pain — Tampa
- Low Back Pain — Orlando
- Low Back Pain — Miami
- Low Back Pain — St. Petersburg
- Concussion — Tampa
- Concussion — Orlando
- Concussion — Miami
- Concussion — St. Petersburg
- Shoulder Injury — Tampa
- Shoulder Injury — Orlando
- Shoulder Injury — Miami
- Shoulder Injury — St. Petersburg
Don’t see your city? View all Florida service areas.
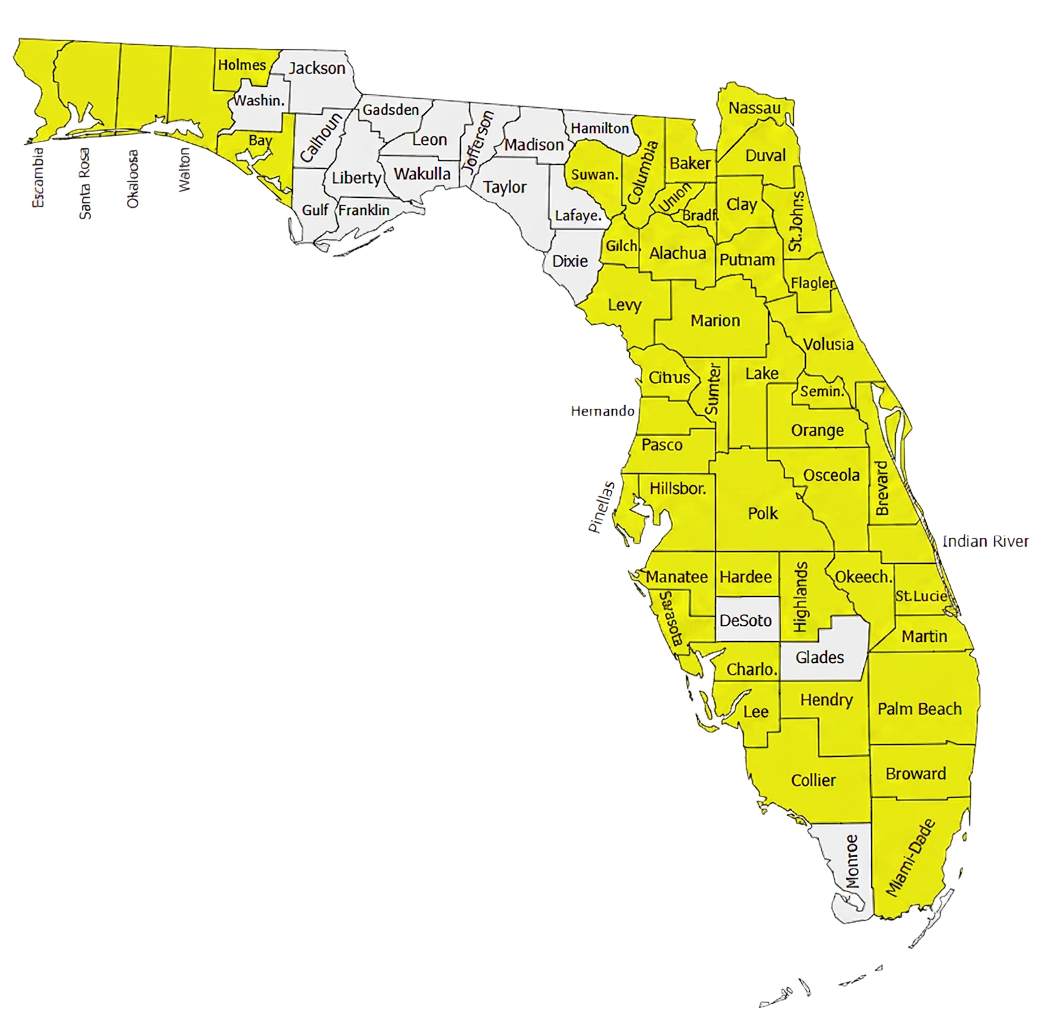
500+ Physical Therapists covering 35+ counties in Florida.
Our clinician network reaches major metros and rural communities alike — from the Panhandle to the Keys. If a patient is in a highlighted county, we can usually see them at home within 24–72 hours of intake.
- Clinicians in network
- 500+
- Florida counties covered
- 35+
Need to refer a Florida patient?
Our intake team confirms PIP and MedPay coverage during the call and schedules most patients for an in-home evaluation within 48 hours.